
Skin cancers are generally classified as 'non-melanoma' or 'melanoma' skin malignancies. The most common ones are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), both categorized as non-melanoma.
Though more commonly found in Caucasians, the fair-skinned, and the red-haired – all who easily burn from sun exposure – skin cancer is increasingly affecting the Malaysian population; which for both sexes ranked 10th against other cancers in the latest (2012-2016) Malaysian National Cancer Registry Report.
The incidence of non-melanoma (NM) skin cancers from the 2012-2016 numbers translates into 1,797 or 3.5 percent in males and 1,395 or 2.2 percent in females, versus 184 males and 163 females with malignant melanoma (MM). Though the number of patients with MM were low, over 70 percent of the cases had been presented late for treatment; with 52-58 percent cases presented at Stage 4 of the disease – a grim prognosis. Despite the lower incidence of MM compared with BCC or SCC, malignant melanoma presents higher mortality in those afflicted by skin cancer, owing to its poor response to conventional adjuvant therapies such as chemotherapy and radiotherapy.

Non-melanoma skin cancers (BCC or SCC) are less aggressive and often are presented in their early stages – more than 50 percent in Stage 1 and eighteen to twenty-one percent in Stage 2. A local five-year study (Han et al., 2019) found NMSC (BCC or SCC) to be often presented in the 8th decade of life and more commonly in the Chinese, followed by the Malays and the Indians. A slightly older study on 32 cases of MM reported over ten years (Pailoor et al., 2012), found 62 percent presented at Stage 3 or 4 and a median age of 62 years. The higher prevalence in the Chinese comes as no surprise given skin cancer’s preferred affliction of the fairer skinned.
In women, malignant melanoma (MM) commonly occurs in the extremities; versus the trunk, head, or neck in men.
Risk Factors
Besides skin fairness (the fairest is called Fitzspatrick type 1), other risk factors to developing MM include increasing age, a history of melanoma, a history of sunburn, and the presence of pre-malignant lesions such as atypical moles – which place about 7 percent of the general population in the risk group for developing malignant melanoma.
Those with atypical mole syndrome, i.e., having more than 100 moles, are twelve times more likely to develop MM. In most cases, the melanoma usually appears as a new lesion rather than rising from pre-existing ones.
Patients with giant hairy moles are at a higher risk of developing malignant melanoma; as high as 40 percent transformation rate has been reported. Sun or ultraviolet (UV) light exposures increase the likelihood of developing malignant melanoma. The risk is higher in cases with a history of extensive exposure/sunburn during childhood.
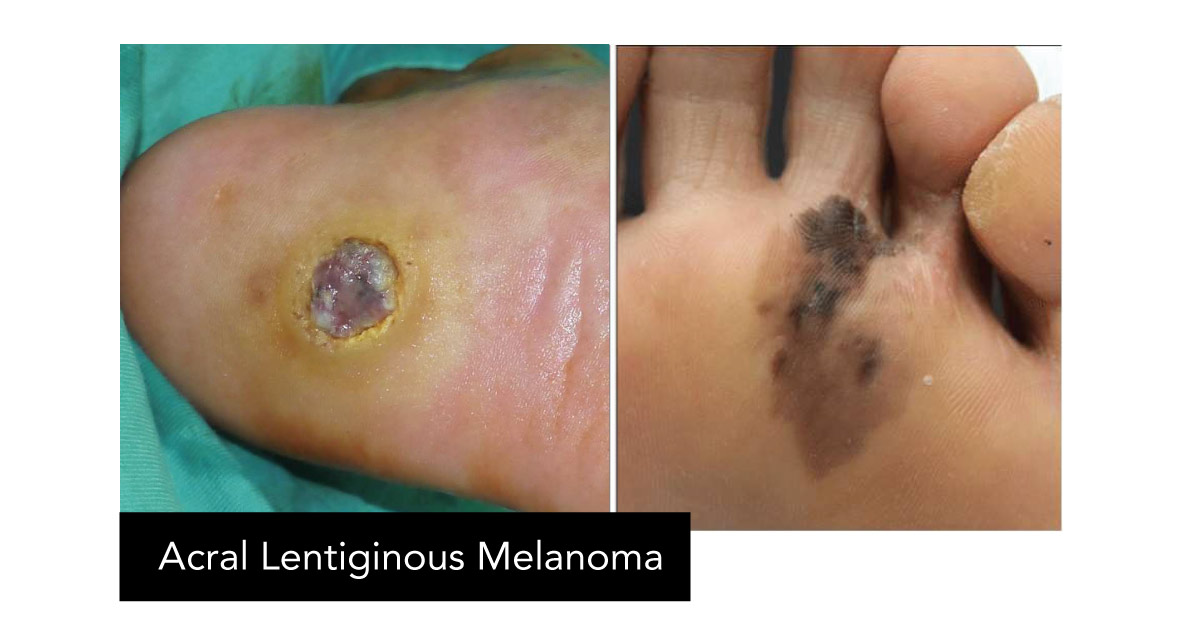
MSU Medical Centre (MSUMC) Plastic and Reconstructive Surgeon Professor Dr Arman Zaharil Mat Saad says that most MM cases treated in Malaysia involve the peripheral/limb areas, are found on the foot sole, and are presented at as late as Stage 3 or 4. The finding was mirrored in the 2012 study by Pailoor et al., which cited 32 cases; 16 on the lower limbs, and 12 on the soles.
What You Can Do
Suspicious of a lesion? See a doctor/specialist of skin cancers – who could be a plastic surgeon, a dermatologist, or an oncology surgeon – for consultation and possible biopsy to obtain a definitive diagnosis.
Once diagnosis is obtained, staging investigation should follow thorough clinical examination to check for enlarged satellite, in-transit, or regional lymph nodes. This is usually done via CT or PET scan, liver-function test, and genetic study of gene mutations (BRAF/KIT).
Treatment
Early-stage treatment may involve surgical resection alone, which may offer a cure for the disease. A sentinel lymph node biopsy may be offered to patients with clinically-negative lymph node to detect early cancer spread or micro-metastasis.
Patients with palpable regional lymph nodes or lymph-nodes detected on the imager/scanner should have a lymph-node biopsy as well as a block dissection of the particular lymphatic basin.
As for adjuvant treatment, new development in systemic therapy using immunotherapy (monoclonal antibodies) and targeted therapy (BRAF / KIT inhibitors) may offer new hope for those with metastatic disease or in an advanced stage of melanoma (in which case chemotherapeutic agents offer little assistance and radiotherapy may only relieve symptoms in patients with metastases to the brain/spine or bones).
MSU Medical Centre is the first specialist hospital in Malaysia built by a private university; situated on campus adjacent to MSU’s student accommodation The Residence.

Management and Science University (MSU) through the MSU International Medical School (IMS) offers Bachelor of Medicine and Bachelor of Surgery (MBBS) at both the main Shah Alam campus in Section 13 and MSU's offshore campus in Bangalore, India.
MSU offers the Diploma in Radiotherapy and the Diploma in Medical Laboratory Technology programmes at the University’s Faculty of Health and Life Sciences (FHLS).

MSU Bachelor of Medical Sciences (Hons)
.jpg)
Skin cancers are generally classified as 'non-melanoma' or 'melanoma' skin malignancies. The most common ones are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), both categorized as non-melanoma.
Though more commonly found in Caucasians, the fair-skinned, and the red-haired – all who easily burn from sun exposure – skin cancer is increasingly affecting the Malaysian population; which for both sexes ranked 10th against other cancers in the latest (2012-2016) Malaysian National Cancer Registry Report.
The incidence of non-melanoma (NM) skin cancers from the 2012-2016 numbers translates into 1,797 or 3.5 percent in males and 1,395 or 2.2 percent in females, versus 184 males and 163 females with malignant melanoma (MM). Though the number of patients with MM were low, over 70 percent of the cases had been presented late for treatment; with 52-58 percent cases presented at Stage 4 of the disease – a grim prognosis. Despite the lower incidence of MM compared with BCC or SCC, malignant melanoma presents higher mortality in those afflicted by skin cancer, owing to its poor response to conventional adjuvant therapies such as chemotherapy and radiotherapy.
Non-melanoma skin cancers (BCC or SCC) are less aggressive and often are presented in their early stages – more than 50 percent in Stage 1 and eighteen to twenty-one percent in Stage 2. A local five-year study (Han et al., 2019) found NMSC (BCC or SCC) to be often presented in the 8th decade of life and more commonly in the Chinese, followed by the Malays and the Indians. A slightly older study on 32 cases of MM reported over ten years (Pailoor et al., 2012), found 62 percent presented at Stage 3 or 4 and a median age of 62 years. The higher prevalence in the Chinese comes as no surprise given skin cancer’s preferred affliction of the fairer skinned.
In women, malignant melanoma (MM) commonly occurs in the extremities; versus the trunk, head, or neck in men.
Risk Factors
Besides skin fairness (the fairest is called Fitzspatrick type 1), other risk factors to developing MM include increasing age, a history of melanoma, a history of sunburn, and the presence of pre-malignant lesions such as atypical moles – which place about 7 percent of the general population in the risk group for developing malignant melanoma.
Those with atypical mole syndrome, i.e., having more than 100 moles, are twelve times more likely to develop MM. In most cases, the melanoma usually appears as a new lesion rather than rising from pre-existing ones.
Patients with giant hairy moles are at a higher risk of developing malignant melanoma; as high as 40 percent transformation rate has been reported. Sun or ultraviolet (UV) light exposures increase the likelihood of developing malignant melanoma. The risk is higher in cases with a history of extensive exposure/sunburn during childhood.
MSU Medical Centre (MSUMC) Plastic and Reconstructive Surgeon Professor Dr Arman Zaharil Mat Saad says that most MM cases treated in Malaysia involve the peripheral/limb areas, are found on the foot sole, and are presented at as late as Stage 3 or 4. The finding was mirrored in the 2012 study by Pailoor et al., which cited 32 cases; 16 on the lower limbs, and 12 on the soles.
What You Can Do
Suspicious of a lesion? See a doctor/specialist of skin cancers – who could be a plastic surgeon, a dermatologist, or an oncology surgeon – for consultation and possible biopsy to obtain a definitive diagnosis.
Once diagnosis is obtained, staging investigation should follow thorough clinical examination to check for enlarged satellite, in-transit, or regional lymph nodes. This is usually done via CT or PET scan, liver-function test, and genetic study of gene mutations (BRAF/KIT).
Treatment
Early-stage treatment may involve surgical resection alone, which may offer a cure for the disease. A sentinel lymph node biopsy may be offered to patients with clinically-negative lymph node to detect early cancer spread or micro-metastasis.
Patients with palpable regional lymph nodes or lymph-nodes detected on the imager/scanner should have a lymph-node biopsy as well as a block dissection of the particular lymphatic basin.
As for adjuvant treatment, new development in systemic therapy using immunotherapy (monoclonal antibodies) and targeted therapy (BRAF / KIT inhibitors) may offer new hope for those with metastatic disease or in an advanced stage of melanoma (in which case chemotherapeutic agents offer little assistance and radiotherapy may only relieve symptoms in patients with metastases to the brain/spine or bones).
MSU Medical Centre is the first specialist hospital in Malaysia built by a private university; situated on campus adjacent to MSU’s student accommodation The Residence.
Management and Science University (MSU) through the MSU International Medical School (IMS) offers Bachelor of Medicine and Bachelor of Surgery (MBBS) at both the main Shah Alam campus in Section 13 and MSU's offshore campus in Bangalore, India.
MSU offers the Diploma in Radiotherapy and the Diploma in Medical Laboratory Technology programmes at the University’s Faculty of Health and Life Sciences (FHLS).
MSU Bachelor of Medical Sciences (Hons)